The Hidden Cost of Poor Clinical Documentation in Optometry
Clinical documentation forms the foundation of defensible, continuous, and evidence-based healthcare delivery.
Clinical documentation forms the foundation of defensible, continuous, and evidence-based healthcare delivery. Within optometry and ophthalmology, accurate documentation is essential not only for continuity of patient care but also for medico-legal protection, inter-professional communication, and regulatory compliance.
Despite its importance, documentation quality remains inconsistent across many independent eye care practices. Paper records, abbreviated notes, missing examination findings, and fragmented patient histories continue to be common operational challenges.
Poor documentation introduces significant risks. These include clinical errors, communication failures, reduced efficiency, reimbursement complications, and medico-legal vulnerability.
The Importance of Structured Documentation
Eye care involves multiple data points including refractive findings, binocular vision assessments, intraocular pressure measurements, retinal imaging, contact lens parameters, and treatment plans. Managing these datasets manually becomes increasingly difficult as patient volumes grow.
Structured documentation improves:
- Clinical consistency
- Diagnostic accuracy
- Continuity of care
- Referral communication
- Treatment monitoring
- Audit readiness
Incomplete documentation can compromise patient safety. Missing progression notes in glaucoma or diabetic retinopathy management may delay intervention and worsen outcomes.
Medico-Legal Considerations
Clinical records serve as legal documents. In disputes involving delayed diagnosis, improper management, or adverse outcomes, documentation becomes the primary evidence of clinical reasoning and patient communication.
Poorly maintained records may be interpreted as negligence or lack of standardization. Common deficiencies include:
- Missing informed consent
- Incomplete history
- Lack of differential diagnosis
- Absent follow-up instructions
- Unclear treatment plans
Digital documentation systems improve defensibility through timestamping, audit logs, and standardized templates.
The Transition from Paper to Digital Systems
Traditional paper-based systems create several operational limitations:
1. Limited accessibility
2. Illegible handwriting
3. Physical storage burdens
4. Difficulty retrieving historical data
5. Inconsistent formatting
6. Increased risk of data loss
Electronic medical records have transformed documentation quality by introducing structured workflows and searchable records.
ASIRA’s Contribution to Documentation Standardization
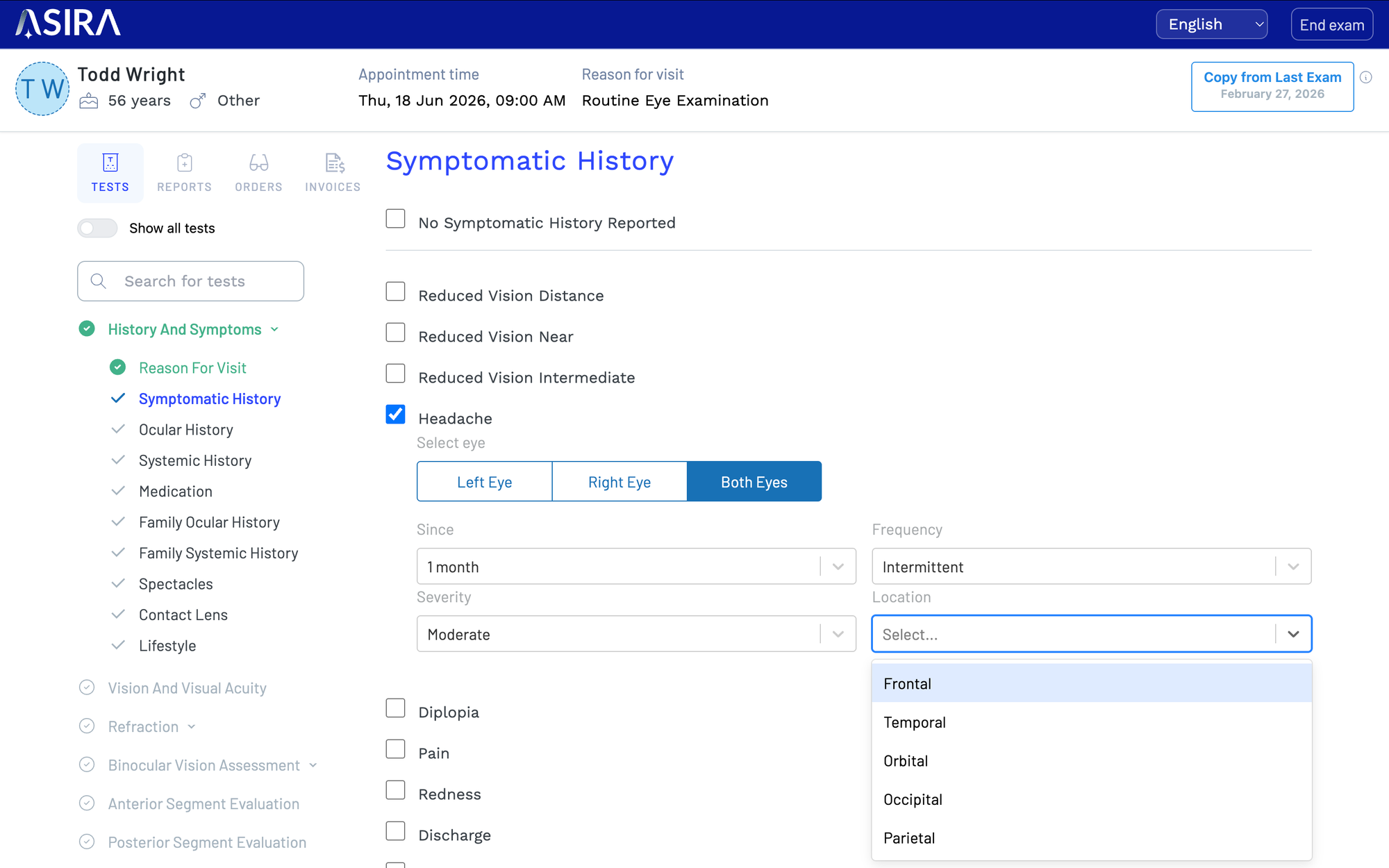
ASIRA has been designed specifically for eye care workflows. The platform allows clinicians to create structured examination templates that standardize record keeping across practitioners and branches.
Features include:
- Customizable examination templates
- Integrated imaging workflows
- Digital prescriptions
- Diagnosis tracking
- Follow-up documentation
- Audit-ready patient timelines
By reducing reliance on freehand notes, ASIRA improves consistency and completeness of records.
Interprofessional Communication
Optometrists increasingly collaborate with ophthalmologists, physicians, endocrinologists, and pediatric specialists. Structured digital records facilitate clearer referrals and improved interdisciplinary communication.
Comprehensive EMR systems allow rapid sharing of findings and treatment history, improving continuity and reducing duplication.
Efficiency and Workflow Optimisation
Clinicians often perceive documentation as time-consuming. However, standardised EMR workflows reduce repetitive data entry and improve operational efficiency.
ASIRA integrates clinical documentation with billing, appointment scheduling, inventory, and communication systems. This reduces workflow fragmentation and administrative duplication.
Data Analytics and Population Health
Digital documentation enables large-scale analysis of patient trends. Clinics can evaluate:
- Disease prevalence
- Prescription trends
- Follow-up compliance
- Optical conversion rates
- Clinical performance indicators
These insights support evidence-based decision-making and practice growth.
Regulatory Implications
As healthcare regulation evolves globally, documentation standards continue to increase. India’s National Commission for Allied and Healthcare Professions (NCAHP) Act represents an important step toward standardisation within optometry.
Structured documentation systems help practices align with evolving professional expectations and accountability frameworks.
Patient Trust and Professionalism
Patients increasingly associate digital systems with professionalism and organized care delivery. Access to digital prescriptions, historical records, and transparent communication improves confidence and satisfaction.
Future Directions
Artificial intelligence may further enhance documentation through voice-assisted charting, automated coding, and clinical decision support systems.
Integrated EMR ecosystems are likely to become essential infrastructure rather than optional tools.
Conclusion
Poor clinical documentation creates hidden operational, financial, and medico-legal costs that many practices underestimate. As optometry continues evolving toward evidence-based and regulated healthcare delivery, standardized digital documentation will become increasingly critical.
ASIRA provides eye care practices with structured, scalable, and clinically oriented documentation tools that improve efficiency, continuity, and accountability.
ASIRA is a simple and secure, cloud-based software tool, that helps eye care professionals reduce the time and effort required to maintain clinical records, schedule appointments, generate bills, manage inventory and much more!
To find out more, visit www.asira.health and sign up for a FREE TRIAL!



Comments ()