Why Every Comprehensive Eye Examination Should Include Dry Eye Screening
Dry eye disease has become one of the most frequently encountered conditions in clinical practice. Yet dry eye remains one of the most underdiagnosed and undertreated conditions by eye care practitioners.

Dry eye disease has become one of the most frequently encountered conditions in clinical practice. It affects millions of people worldwide, influences quality of life to a degree comparable with many systemic chronic diseases, and represents a significant burden on both patients and healthcare systems. Yet despite its prevalence, dry eye remains one of the most underdiagnosed and undertreated conditions encountered by eye care practitioners.
One of the greatest challenges in managing dry eye disease is that it rarely presents in a predictable way. Some patients arrive complaining of burning, irritation, fluctuating vision and excessive tearing, while others with significant ocular surface disease report few or no symptoms at all. A patient attending for a routine eye examination may show clear evidence of meibomian gland dysfunction, reduced tear film stability or corneal staining despite believing their eyes are perfectly healthy.
For many years, dry eye was considered a relatively simple condition caused by inadequate tear production. Artificial tears were often prescribed, symptoms temporarily improved, and both practitioner and patient moved on. Today, we know that the condition is far more complex.
Over the past two decades, our understanding of dry eye disease has undergone a remarkable transformation. This shift has been driven largely by the Tear Film and Ocular Surface Society (TFOS), whose Dry Eye Workshop (DEWS) reports have become the international gold standard for the diagnosis and management of dry eye disease. The publication of TFOS DEWS I in 2007 fundamentally changed how clinicians viewed dry eye. A decade later, TFOS DEWS II incorporated an enormous body of new evidence, redefining dry eye as a multifactorial disease characterised by the loss of tear film homeostasis. Most recently, TFOS DEWS III has refined these recommendations further, integrating the latest evidence on diagnosis, pathophysiology and management while reinforcing the importance of personalised, evidence-based care. Together, these three reports tell an important story. Dry eye disease is no longer viewed simply as a deficiency of tears. It is recognised as a chronic disease of the ocular surface that requires systematic assessment, careful documentation and long-term management.
For optometrists, this has important implications. If dry eye disease is common, progressive and frequently underdiagnosed, then waiting for patients to complain before looking for it is no longer sufficient. Instead, every comprehensive eye examination should include some level of dry eye assessment. Doing so not only improves the likelihood of early diagnosis but also allows practitioners to identify risk factors, establish baseline findings and intervene before significant ocular surface damage develops.
A disease hiding in plain sight
Dry eye disease is estimated to affect between 5% and 50% of the global population, depending on the diagnostic criteria used and the population being studied. Prevalence continues to increase with age, although younger patients are now being diagnosed with increasing frequency due to prolonged digital device use, environmental factors and lifestyle changes.
Many of these patients present to optometrists for entirely unrelated reasons. A child attending for a myopia assessment, an adult seeking new spectacles or a diabetic patient attending for retinal screening may all have clinically significant ocular surface disease that has never previously been recognised. This is one of the central messages that has emerged from successive TFOS reports.
Dry eye disease should not simply be investigated when symptoms are reported. Instead, clinicians should actively look for evidence of ocular surface disease as part of a comprehensive examination for the following reasons:
- Patients can be educated before symptoms become debilitating.
- Lifestyle and environmental modifications can be introduced early.
- Meibomian gland dysfunction can be identified before irreversible gland dropout occurs.
- Clinicians establish a valuable clinical baseline against which future progression can be monitored.
How our understanding of dry eye has evolved
One of the most fascinating aspects of dry eye research is how dramatically our understanding has changed over the past twenty years.
TFOS DEWS I (2007): Recognising complexity
Before the publication of TFOS DEWS I, dry eye was commonly viewed as a disorder caused primarily by insufficient tear production. Although evaporative causes were recognised, clinical management often focused heavily on replacing tears with lubricants.
TFOS DEWS I challenged this simplified view. For the first time, dry eye disease was formally defined as a multifactorial disease of the tears and ocular surface, characterised by symptoms of discomfort, visual disturbance, tear film instability and potential damage to the ocular surface. The report also recognised the roles of increased tear osmolarity and inflammation, concepts that have since become central to modern dry eye management.
Importantly, TFOS DEWS I highlighted that successful management required clinicians to look beyond symptoms alone and consider the complex interaction between the tear film, eyelids, ocular surface and environment. This marked the beginning of a significant shift in clinical thinking.
TFOS DEWS II (2017): Introducing tear film homeostasis
Ten years later, TFOS DEWS II built upon several more recent publications and introduced one of the most influential concepts in modern ocular surface disease: tear film homeostasis.
Rather than defining dry eye simply by reduced tear volume or patient symptoms, DEWS II described dry eye as:
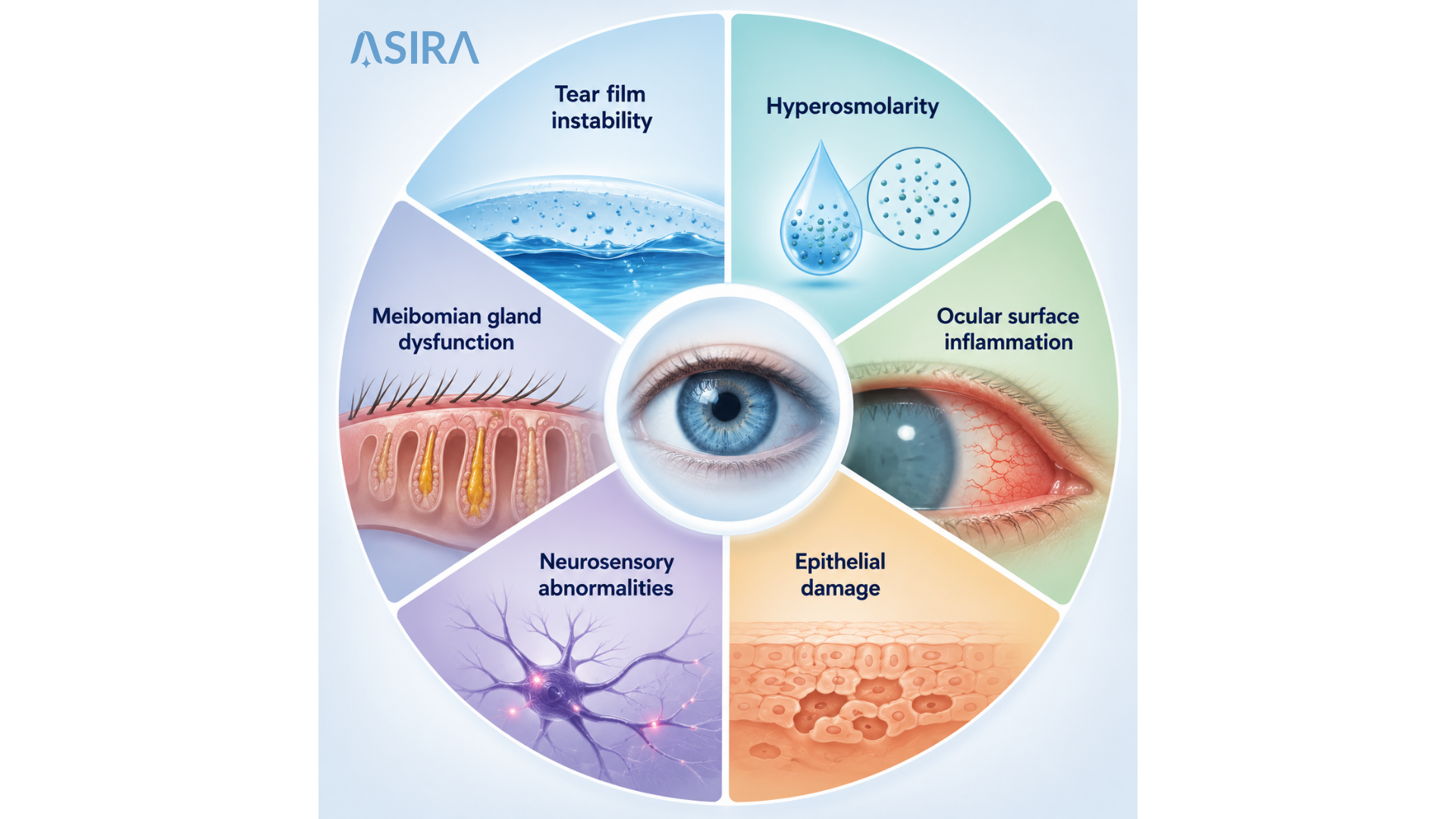
"A multifactorial disease of the ocular surface characterised by a loss of homeostasis of the tear film, accompanied by ocular symptoms, in which tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities play aetiological roles."
This definition fundamentally changed clinical practice. It recognised that multiple interconnected mechanisms contribute to disease, including:
Rather than searching for a single cause, clinicians were encouraged to identify which mechanisms were contributing to an individual patient's disease and tailor management accordingly. Equally important, TFOS DEWS II proposed structured diagnostic algorithms, emphasising the use of validated symptom questionnaires alongside objective clinical tests. For many practitioners, this represented a move towards a far more standardised and evidence-based approach to dry eye assessment.
TFOS DEWS III (2025): Refining diagnosis and embracing personalised care
The publication of TFOS DEWS III represents the next chapter in the evolution of dry eye management. Rather than replacing DEWS II, it builds upon its foundations, incorporating almost another decade of scientific discovery and clinical experience.
One of the most important messages throughout the DEWS III reports is that dry eye disease should not be approached as a single condition with a standard treatment pathway. Instead, clinicians should identify the specific mechanisms driving disease in each patient and develop an individualised management plan.
The report places even greater emphasis on:
- Early diagnosis before significant ocular surface damage occurs
- Standardised, evidence-based diagnostic pathways
- Identification of disease subtype and severity
- Longitudinal monitoring of disease progression
- Patient education and shared decision-making
- Personalised treatment strategies rather than a "one-size-fits-all" approach
Perhaps most importantly, DEWS III recognises that dry eye disease is dynamic. The ocular surface changes over time, patient symptoms fluctuate, treatment responses vary, and management plans often need adjustment. This reinforces the importance of maintaining detailed clinical records that allow practitioners to compare findings between visits and monitor disease progression objectively. For optometrists, this means that every consultation contributes to a much larger clinical picture. A single examination provides only a snapshot, whereas structured documentation creates a timeline that supports better long-term decision-making.
Why symptoms alone are not enough
One of the most consistent findings throughout the TFOS reports is the surprisingly poor relationship between symptoms and clinical signs. This may seem counterintuitive. As clinicians, we often expect patients with severe disease to report significant symptoms and those with mild disease to report very little discomfort. Dry eye disease rarely follows this pattern.
Many practitioners have encountered patients with severe meibomian gland dysfunction, marked tear film instability and significant corneal staining who insist that their eyes feel perfectly comfortable. Equally, some patients report debilitating discomfort despite relatively modest clinical findings. This apparent contradiction can largely be explained by the complex nature of the disease. Tear film instability, inflammation, corneal nerve changes and neurosensory abnormalities all influence how patients perceive ocular discomfort. As a result, symptoms alone cannot reliably determine either the presence or severity of disease.
This is precisely why TFOS recommends combining validated symptom questionnaires with objective clinical assessment. A patient may score highly on the Ocular Surface Disease Index (OSDI) or the Dry Eye Questionnaire-5 (DEQ-5), highlighting significant symptoms that warrant further investigation. Conversely, a patient with few symptoms may still demonstrate reduced tear break-up time, lid margin abnormalities or meibomian gland dysfunction during routine examination. Without actively looking for these findings, early disease may remain undetected for years.
Dry eye screening should become part of every comprehensive eye examination
As our understanding of dry eye disease has evolved, so too has the role of the comprehensive eye examination. Traditionally, dry eye investigations were often reserved for symptomatic patients or those specifically requesting treatment. Modern evidence suggests this approach risks missing a substantial proportion of patients with clinically significant disease. Routine dry eye screening does not require an extensive battery of specialist investigations for every patient. Instead, it involves incorporating a systematic assessment of the ocular surface into every comprehensive examination.
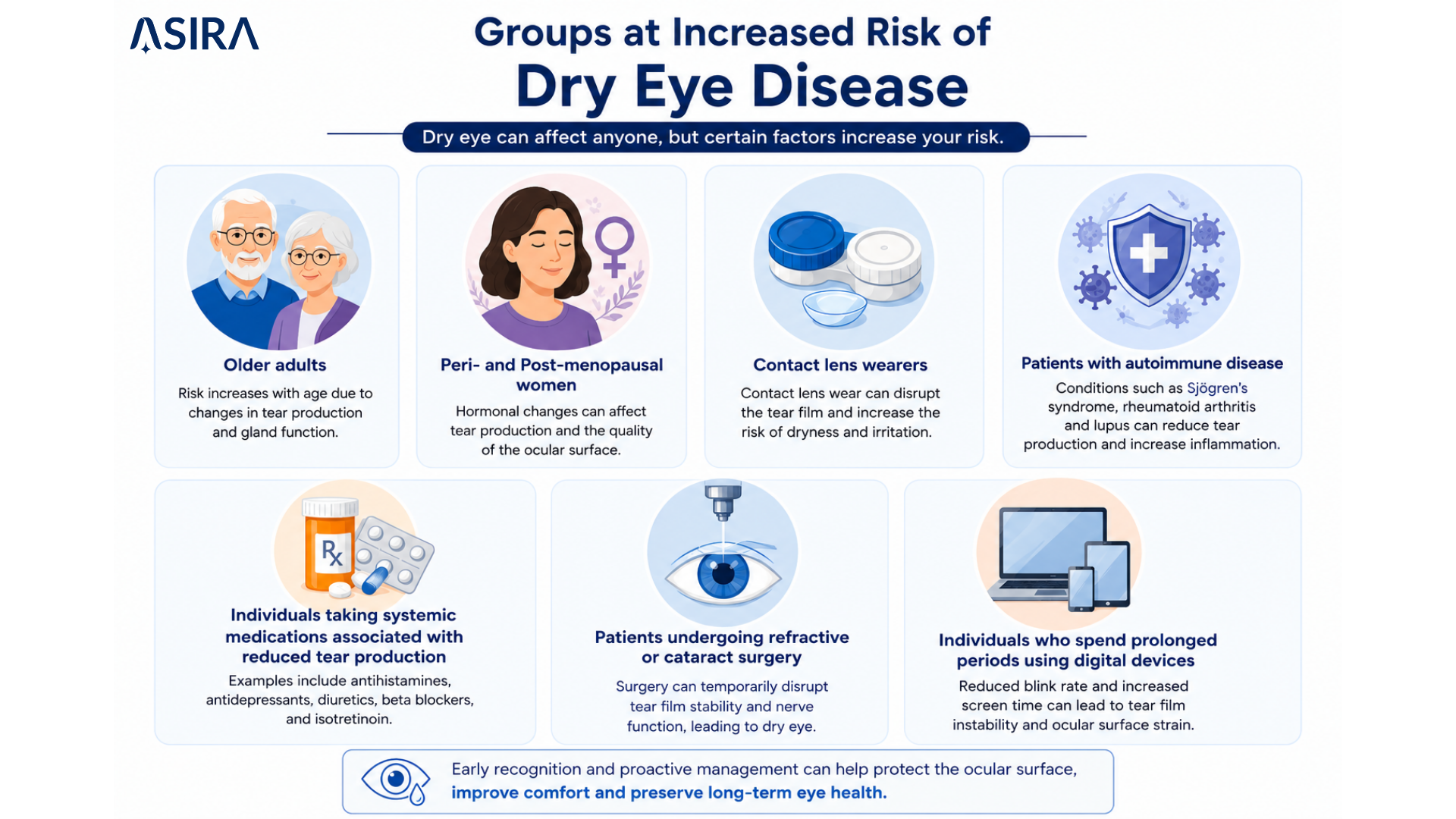
This begins with recognising risk factors. Age, hormonal changes, autoimmune disease, diabetes, contact lens wear, prolonged digital device use, refractive surgery, systemic medications and environmental exposures all increase the likelihood of dry eye disease. A thorough history should therefore include targeted questions relating to symptoms, occupational demands, screen use, medications and previous ocular interventions. Validated symptom questionnaires such as the OSDI or DEQ-5 provide a structured method of quantifying symptom severity while establishing an objective baseline that can be monitored over time.
Clinical assessment should then include examination of both the tear film and ocular surface. Although the exact examination sequence may vary between practices, the TFOS reports consistently recommend evaluation of:
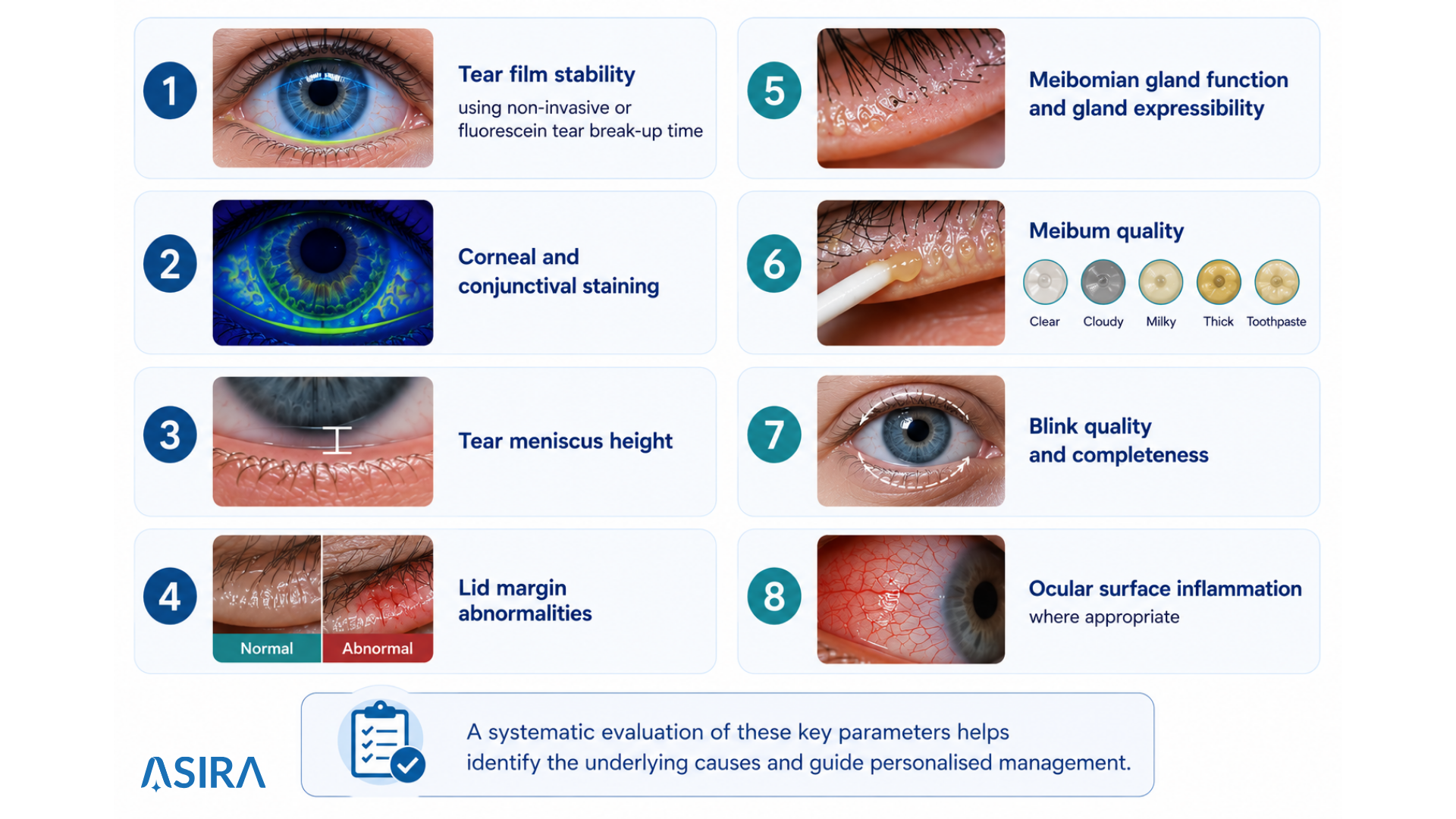
Where available, technologies such as meibography, interferometry and tear osmolarity testing provide additional objective information that may assist diagnosis and monitoring.
Importantly, the examination should not end once a diagnosis has been made. Dry eye disease is chronic. Every consultation should establish a baseline that allows meaningful comparison during future visits.
The importance of documenting what you find
Accurate diagnosis is only one component of effective dry eye management. Equally important is the ability to document findings consistently. Consider two patients with moderate evaporative dry eye disease, both attend six months later following treatment. One clinician relies entirely on memory and brief handwritten notes. The other has access to detailed documentation of tear break-up time, meibomian gland grading, staining patterns, symptom scores, eyelid photographs and previous management strategies.
Which practitioner is better positioned to judge whether treatment has been successful? The answer is obvious. Structured documentation transforms isolated consultations into continuous clinical care. It allows practitioners to recognise subtle changes, monitor progression, evaluate treatment effectiveness and communicate findings more clearly with patients. It also improves consistency across practices with multiple clinicians. Regardless of who performs the follow-up examination, every practitioner has access to the same structured clinical information. This level of consistency is becoming increasingly important as dry eye management becomes more sophisticated and more personalised.
Turning international guidelines into everyday clinical practice
The TFOS reports provide an outstanding evidence base, but translating several hundred pages of consensus recommendations into a busy clinical workflow is not always straightforward. This is where thoughtfully designed clinical templates become invaluable.
At ASIRA, our Dry Eye Template was developed around the principles established by TFOS DEWS I, refined through the recommendations of TFOS DEWS II and continually updated to reflect emerging evidence, including the latest concepts presented in TFOS DEWS III. Rather than relying on memory alone, the template guides practitioners through a systematic examination that mirrors internationally accepted best practice.
Because every examination follows the same logical sequence, important findings are far less likely to be overlooked. The template also supports longitudinal care by allowing clinicians to compare findings across multiple visits. Changes in symptom scores, tear film stability, staining patterns and gland function become immediately visible, helping practitioners determine whether treatment is effective or requires modification.
Clinical images, slit lamp photographs and meibography can be stored alongside examination findings, creating a comprehensive record that supports both clinical decision-making and patient education. Perhaps one of its greatest strengths is consistency. Whether a patient is examined by one practitioner or several members of the same clinical team, structured documentation ensures that everyone is speaking the same clinical language.
In this way, the ASIRA Dry Eye Template does far more than simplify record keeping. It helps translate internationally recognised evidence into practical, repeatable clinical care that benefits both practitioners and patients alike.
Better documentation creates better conversations
One of the most overlooked benefits of structured dry eye documentation is the impact it has on communication. Patients often struggle to understand concepts such as tear film instability, gland dysfunction or ocular surface inflammation because these changes cannot be seen or felt directly. However, when practitioners can display previous slit lamp photographs, meibography images or symptom trends over time, the conversation changes. Instead of saying, "Your dry eye looks slightly better today," the clinician can show exactly how staining has reduced or gland function has improved. Objective evidence transforms abstract explanations into meaningful discussions and patients become active participants in their care rather than passive recipients of treatment recommendations. The role of the practitioner is no longer simply to diagnose disease but to educate, guide and empower patients to manage chronic conditions successfully.
Conclusion
Dry eye disease has undergone one of the most significant paradigm shifts in modern eye care. What was once considered a relatively straightforward disorder of tear deficiency is now recognised as a complex, multifactorial disease of the ocular surface involving tear film instability, inflammation, neurosensory abnormalities and disruption of ocular surface homeostasis. The publication of TFOS DEWS I, TFOS DEWS II and, most recently, TFOS DEWS III has fundamentally changed the way clinicians approach diagnosis and management. Routine screening enables earlier diagnosis, identifies patients who may otherwise remain undetected and allows practitioners to intervene before significant ocular surface damage develops. Equally important, dry eye should be viewed as a chronic disease requiring ongoing monitoring rather than episodic treatment.
Consistent documentation, objective assessment and patient education are now central components of evidence-based care. At ASIRA, these principles have shaped the design of our Dry Eye Template from the very beginning. Rather than creating another electronic form, we set out to develop a workflow that reflects internationally recognised best practice. Built around the recommendations of the TFOS DEWS reports, the template guides practitioners through a comprehensive, structured assessment while remaining flexible enough to suit individual styles of practice. By incorporating validated symptom questionnaires, detailed ocular surface assessment, meibomian gland evaluation, clinical imaging and longitudinal monitoring into a single workflow, ASIRA helps practitioners translate international evidence into everyday clinical practice. Ultimately, technology should never replace clinical judgement, its role is to support it.
When evidence-based guidelines are combined with thoughtful clinical reasoning and consistent documentation, practitioners are better equipped to deliver personalised care, monitor disease progression and improve long-term outcomes for every patient living with dry eye disease.
References
- Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II Definition and Classification Report. Ocul Surf. 2017;15(3):276-283.
- Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II Diagnostic Methodology Report. Ocul Surf. 2017;15(3):539-574.
- Jones L, Downie LE, Korb D, et al. TFOS DEWS II Management and Therapy Report. Ocul Surf. 2017;15(3):575-628.
- Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II Epidemiology Report. Ocul Surf. 2017;15(3):334-365.
- Baudouin C, Messmer EM, Aragona P, et al. TFOS DEWS II Pathophysiology Report. Ocul Surf. 2017;15(3):438-510.
- The Tear Film & Ocular Surface Society (TFOS). TFOS DEWS III Report. The Ocular Surface. 2025. (Collection of consensus reports.)
- Lemp MA, Baudouin C, Baum J, et al. The Definition and Classification of Dry Eye Disease. Report of the International Dry Eye Workshop (DEWS). Ocul Surf. 2007;5(2):75-92.
- Nelson JD, Shimazaki J, Benitez-del-Castillo JM, et al. The International Workshop on Meibomian Gland Dysfunction. Invest Ophthalmol Vis Sci. 2011;52(4):1930-1937.
- Nichols KK, Foulks GN, Bron AJ, et al. The International Workshop on Meibomian Gland Dysfunction: Executive Summary. Invest Ophthalmol Vis Sci. 2011;52(4):1922-1929.
- Bron AJ, de Paiva CS, Chauhan SK, et al. TFOS DEWS II Pathophysiology Report. Ocul Surf. 2017;15(3):438-510.
- Sullivan BD, Crews LA, Messmer EM, et al. Correlations between commonly used objective signs and symptoms for the diagnosis of dry eye disease. Acta Ophthalmol. 2014;92:e161-e166.
- Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the Ocular Surface Disease Index (OSDI). Arch Ophthalmol. 2000;118(5):615-621.
- Chalmers RL, Begley CG, Caffery B. Validation of the Dry Eye Questionnaire (DEQ-5). Cornea. 2010;29(10):1120-1126.
- Bron AJ, Tiffany JM. The contribution of meibomian disease to dry eye. Ocul Surf. 2004;2(2):149-165.
- Craig JP, Nelson JD, Azar DT, et al. TFOS Lifestyle Report. Ocul Surf. 2023.
- Nichols KK, et al. TFOS Lifestyle Workshop Executive Summary. Ocul Surf. 2023.
- Baudouin C. The pathology of dry eye. Surv Ophthalmol. 2001;45(Suppl 2):S211-S220.
- American Academy of Ophthalmology Preferred Practice Pattern®. Dry Eye Syndrome. Latest edition.
- Jones L, et al. TFOS DEWS II Executive Summary. Ocul Surf. 2017;15(4):802-812.
- Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II Executive Summary. Ocul Surf. 2017;15(4):802-812.
ASIRA is a cloud-based EMR and practice management software built by eye care professionals for eye care professionals. We have helped hundreds of practices change the way they work. To find out more, visit www.asira.health and sign up for a FREE TRIAL!



Comments ()