Current Evidence, Optical Principles, and Clinical Application for Myopia Control Spectacle Lenses.
Myopia is increasingly recognised as a significant public health concern, with projections suggesting that nearly half of the global population may be affected by 2050.

Introduction
Myopia is increasingly recognised as a significant public health concern, with projections suggesting that nearly half of the global population may be affected by 2050. The clinical importance lies not only in refractive error, but in the associated risk of long-term ocular morbidity, including myopic maculopathy and retinal detachment.
Once myopia develops, the primary therapeutic objective is to reduce the rate of progression, typically quantified through changes in spherical equivalent refraction (SER) and axial length (AL). Among the available interventions, spectacle lenses remain a widely accessible and non-invasive option, particularly in paediatric populations.
Recent advances in optical design have led to the development of three principal categories of myopia control spectacle lenses:
Defocus Incorporated Multiple Segments (DIMS), Highly Aspherical Lenslet Target (HALT), and Cylindrical Annular Refractive Elements (CARE). While these designs share a common theoretical basis, their optical implementations differ substantially, with implications for both efficacy and clinical use.
Optical Rationale
Conventional single vision (SV) spectacle lenses provide uniform refractive correction across the visual field. While this effectively restores central visual acuity, it does not address peripheral optics. Specifically, SV correction is associated with relative peripheral hyperopic defocus, a condition hypothesised to stimulate axial elongation and contribute to myopia progression.
Contemporary myopia control lenses aim to counter this by introducing peripheral myopic defocus, thereby altering the retinal image profile in a manner that is believed to inhibit axial growth.
However, it is important to recognise that the therapeutic effect is not determined solely by the presence of defocus, but also by the spatial distribution, magnitude, and optical quality of the retinal image. It is within this context that the distinctions between DIMS, HALT, and CARE become clinically relevant.
Spectacle Lens Designs
Defocus Incorporated Multiple Segments (DIMS)
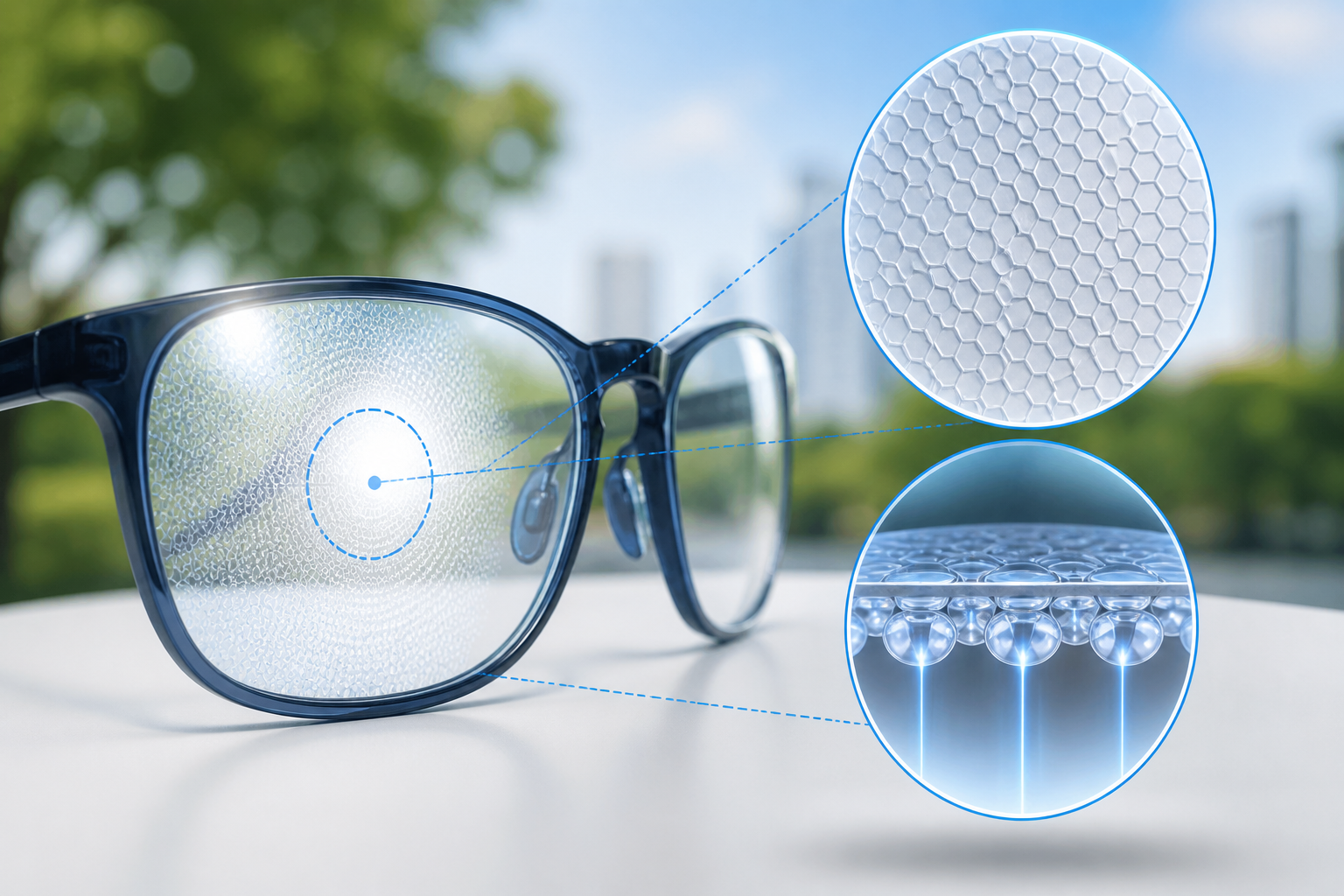
DIMS lenses employ a dual-zone design consisting of a central optical zone for distance correction and a surrounding annular treatment zone composed of multiple discrete lenslets. These lenslets provide approximately +3.50 D of additional power, arranged in a high-density honeycomb configuration.
This design generates simultaneous focused and defocused retinal images, producing a consistent peripheral myopic defocus signal regardless of gaze direction.
From a clinical perspective, DIMS represents a relatively well-characterised system, supported by multiple randomised controlled trials and longitudinal data extending up to six years. Visual function is generally preserved, although transient symptoms such as peripheral blur or visual discomfort have been reported during the adaptation phase.
Highly Aspherical Lenslet Target (HALT)
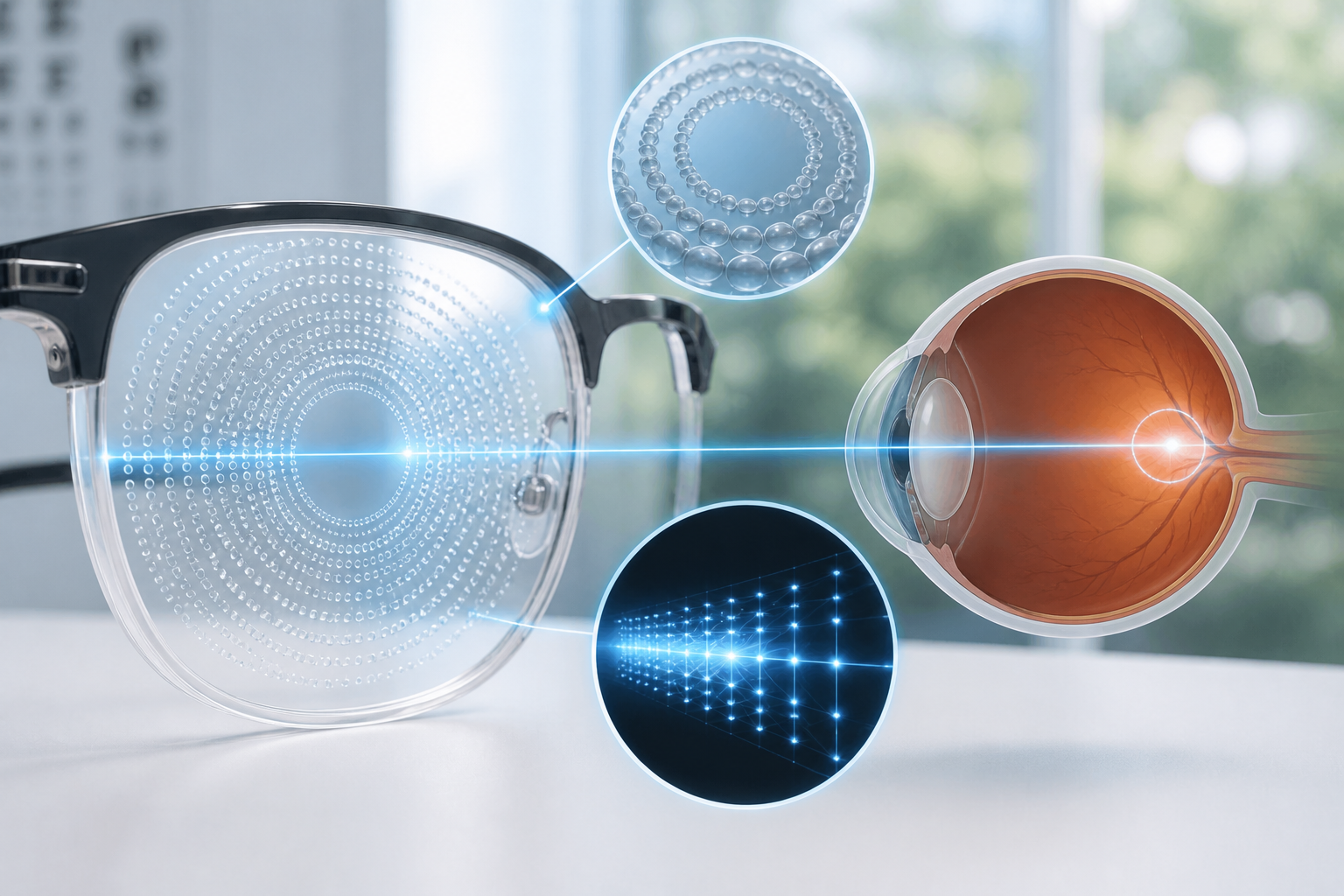
HALT lenses utilise an array of highly aspherical lenslets arranged in concentric rings around a central clear zone. Unlike DIMS, which produces discrete focal planes, HALT generates a three-dimensional distribution of light in front of the retina, often described as a “volume of myopic defocus.”
This approach results in a more continuous defocus profile, which may influence retinal image processing differently compared to segmented designs.
Randomised controlled trials have demonstrated substantial reductions in both SER progression and axial elongation with HALT lenses, with efficacy comparable to, and in some studies exceeding, that observed with DIMS.
Cylindrical Annular Refractive Elements (CARE)
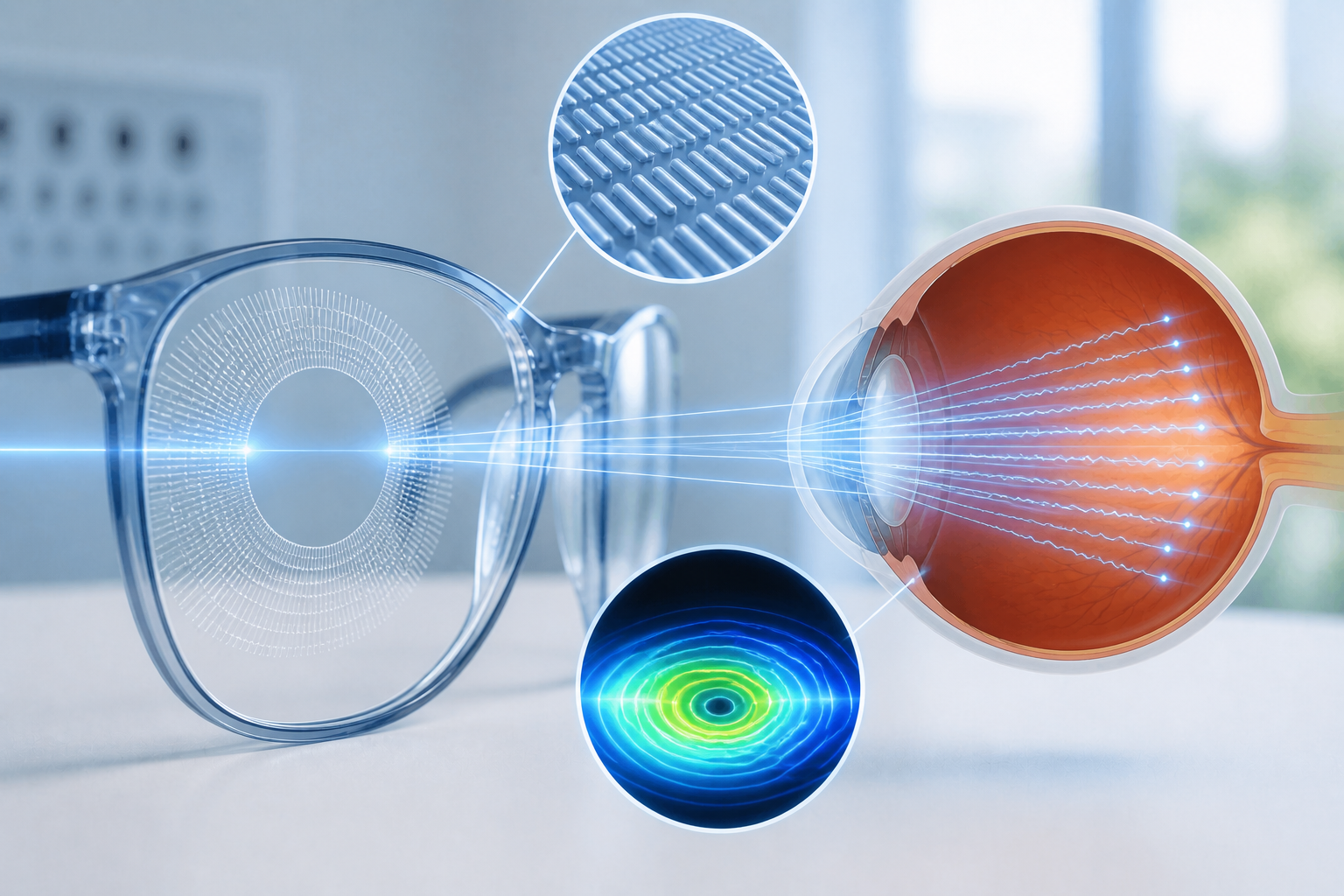
CARE lenses adopt a distinct optical strategy. Rather than relying solely on spherical defocus, they incorporate annular arrays of micro-cylindrical elements that alter the phase of incoming light. This results in peripheral image degradation through wavefront disruption, rather than the creation of discrete defocused focal points.
The clinical implication of this approach is that the retinal signal is generated through changes in image quality and contrast, rather than conventional defocus mechanisms.
While CARE lenses have demonstrated efficacy in reducing myopia progression, available data suggest that their effect size may be modestly lower compared to DIMS and HALT in direct comparative settings.
Comparative Efficacy
A recent prospective, double-blinded, randomised clinical trial provides the most direct comparison of these three designs. Over a one-year period, all three lens types significantly reduced the rate of myopia progression.
The reported reductions were approximately:
- 56.7% for DIMS
- 58.1% for HALT
- 47% for CARE
No statistically significant difference was observed between DIMS and HALT, whereas both demonstrated superior performance relative to CARE for certain outcome measures.
Importantly, no adverse safety signals were identified, supporting the clinical use of all three designs.
Clinical Interpretation
The observed differences in efficacy are likely attributable to variations in optical signal delivery to the retina. Specifically, differences in lenslet geometry, defocus magnitude, and image quality degradation may influence the strength and consistency of the inhibitory signal for axial growth.
DIMS and HALT, which generate more structured and sustained myopic defocus, may provide a more robust stimulus. In contrast, CARE lenses, which rely on phase disruption, may produce a less uniform or less potent signal.
However, these differences should be interpreted within the context of overall treatment effect, as all three designs provide clinically meaningful reductions in progression compared to single vision correction.
Clinical Application
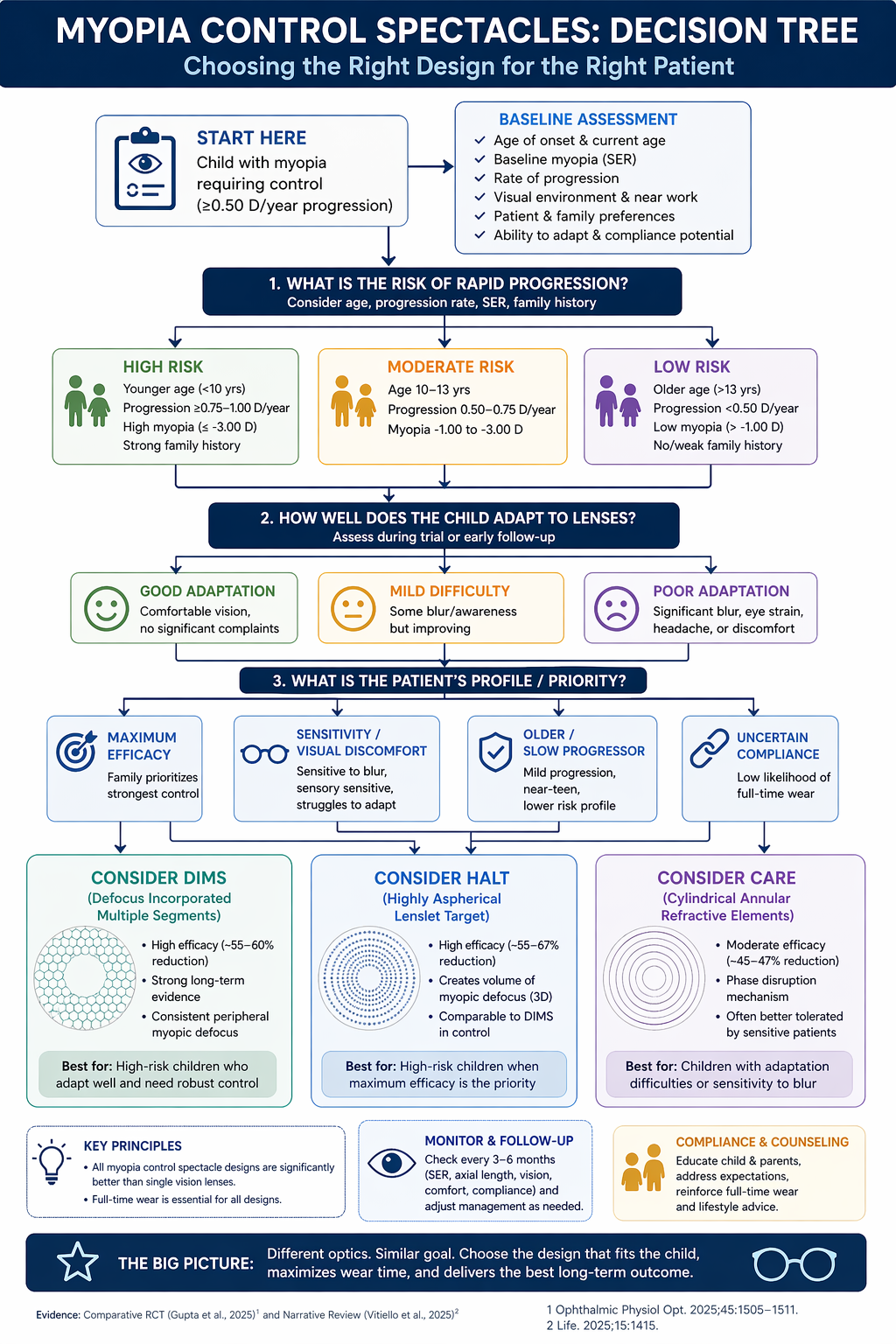
In clinical practice, lens selection should be guided by patient-specific factors rather than a purely design-centric approach.
Patients demonstrating rapid progression, earlier age of onset, or significant familial risk may benefit from designs associated with higher efficacy, such as DIMS or HALT.
Conversely, in patients who report difficulty adapting to lens-induced blur or visual disturbances, alternative designs such as CARE may be considered, particularly if tolerability becomes a limiting factor.
In older children or those with slower progression rates, the relative differences in efficacy may be less clinically significant, and factors such as comfort, cost, and compliance may assume greater importance.
It should also be emphasised that treatment success is highly dependent on consistent wear. Even the most effective optical design is unlikely to yield meaningful benefit in the absence of adequate compliance.
Conclusion
The current evidence supports the use of DIMS, HALT, and CARE spectacle lenses as effective interventions for slowing myopia progression in children.
While these designs share a common theoretical foundation, their differing optical strategies result in measurable differences in clinical performance. DIMS and HALT appear to offer comparable and, in some cases, superior efficacy relative to CARE; however, all three designs provide significant benefit compared to single vision lenses.
The emphasis in contemporary practice should therefore shift from determining whether these lenses are effective, to understanding how best to individualise lens selection based on patient characteristics, visual tolerance, and expected compliance.
Ultimately, the choice of lens should be guided not only by optical design, but by its suitability for the individual patient in a real-world clinical context.
To Book a Demo or to learn more, contact ASIRA at contact@asira.health or via WhatsApp: +919152391194.
Learn more about ASIRA at www.asira.health



Comments ()